
Dutasteride vs Hair Loss & BPH Treatments Comparison Tool
Dutasteride
Finasteride
Minoxidil
Saw Palmetto
Recommendation Based on Your Inputs:
Select your primary concern and budget constraint to get personalized recommendations.
When you’re trying to decide whether Dutanol (dutasteride) is the right choice, you end up weighing a mix of effectiveness, safety, cost, and the specific condition you want to treat. Below you’ll find a side‑by‑side look at dutasteride and the most common alternatives, so you can figure out which drug fits your goals without wading through vague marketing copy.
Quick Summary
- Dutasteride blocks both type I and II 5‑alpha‑reductase enzymes, giving it a broader reach than finasteride.
- Finasteride works well for early‑stage hair loss but is less potent for enlarged prostate.
- Minoxidil is a topical vasodilator; it doesn’t touch hormones but can boost hair density.
- Saw palmetto offers a natural, mild enzyme‑inhibiting effect but lacks strong clinical proof.
- Cost, side‑effect profile, and prescription requirements vary widely - choose based on your health priorities.
What is Dutanol (dutasteride)?
Dutasteride is a synthetic 5‑alpha‑reductase inhibitor originally approved for benign prostatic hyperplasia (BPH). In the UK it’s marketed under brand names like Avodart for BPH and, off‑label, for androgenetic alopecia (male‑pattern hair loss). The drug blocks the conversion of testosterone to dihydrotestosterone (DHT) by inhibiting both type I and type II isoenzymes, which is why many clinicians consider it a more powerful option than finasteride.
How does dutasteride work?
By reducing DHT levels throughout the body, dutasteride slows the miniaturisation of hair follicles and relaxes prostate muscle tone. Lower DHT means fewer hair‑loss signals and less pressure on the urethra, translating into both thicker scalp hair and improved urinary flow for BPH patients.
Key alternatives to consider
Finasteride
Finasteride is another oral 5‑alpha‑reductase inhibitor but it only targets the type II isoenzyme. It’s sold as Propecia for hair loss and Proscar for BPH. Because its enzymatic scope is narrower, finasteride typically reduces scalp DHT by about 70% versus roughly 90% with dutasteride.
Minoxidil
Minoxidil is a topical vasodilator originally used for hypertension. When applied to the scalp at 2% or 5% concentrations, it stimulates hair follicles by increasing blood flow and prolonging the anagen (growth) phase. It doesn’t affect hormone levels, making it a good adjunct if you’re worried about sexual side effects.
Saw Palmetto
Saw Palmetto is a plant extract that weakly inhibits 5‑alpha‑reductase. Some small trials suggest modest DHT reduction, but the evidence is far less consistent than for prescription drugs. Users often appreciate its over‑the‑counter availability and low cost.
Side‑effect landscape
All hormone‑modifying agents share a core set of potential adverse events: decreased libido, erectile dysfunction, and ejaculatory disorders. Dutasteride, because it suppresses DHT more completely, can present a slightly higher incidence of these symptoms. Finasteride’s side‑effect rate sits just under 10% in large FDA‑tracked cohorts. Minoxidil’s most common complaints are scalp irritation and unwanted facial hair. Saw palmetto is generally well tolerated, but rare cases of gastrointestinal upset have been reported.
Cost and accessibility
In the UK, dutasteride costs roughly £30‑£45 for a 30‑day supply on the NHS when prescribed for BPH; off‑label hair‑loss prescriptions may require private payment, pushing the price to £70‑£90. Finasteride is cheaper-about £15‑£25 per month on the NHS. Minoxidil formulations range from £10 for a generic 2% foam to £30 for branded 5% spray. Saw palmetto supplements sell for £8‑£12 per month.
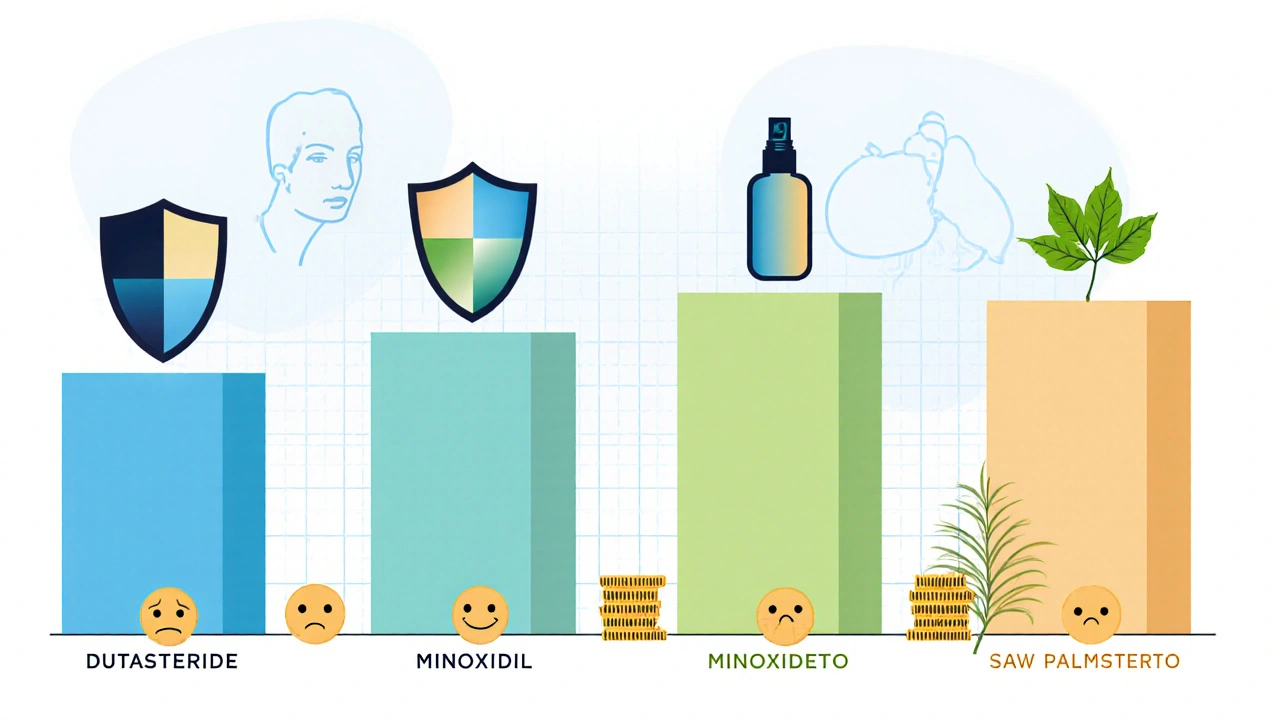
Comparison table
| Attribute | Dutasteride (Dutanol) | Finasteride | Minoxidil | Saw Palmetto |
|---|---|---|---|---|
| Drug class | 5‑alpha‑reductase inhibitor (type I+II) | 5‑alpha‑reductase inhibitor (type II only) | Topical vasodilator | Botanical extract (weak inhibitor) |
| Primary indications | BPH, off‑label hair loss | BPH, hair loss | Androgenetic alopecia | Adjunct for hair loss |
| Typical dose | 0.5mg oral daily | 1mg oral daily (hair loss) / 5mg (BPH) | 2% or 5% solution applied twice daily | 320mg oral daily |
| Hair‑regrowth efficacy* | ≈30‑45% increase in hair count | ≈25‑35% increase | ≈10‑25% increase | ≈5‑15% increase (variable) |
| Common side effects | Sexual dysfunction, breast tenderness, rare depression | Sexual dysfunction, decreased PSA | Scalp irritation, unwanted facial hair | GI upset, mild headache |
| Cost (UK, 30‑day supply) | £30‑£90 (private for hair loss) | £15‑£25 (NHS) / £30‑£45 (private) | £10‑£30 | £8‑£12 |
*Numbers drawn from pooled clinical trials and meta‑analyses up to 2024.
Decision‑making guide
Use the following checklist to match your priorities with the right drug:
- Goal: If you need a single pill that tackles both an enlarged prostate and receding hairline, dutasteride is the only option that covers both.
- Safety first: If sexual side‑effects are a dealbreaker, start with minoxidil or saw palmetto before moving to oral inhibitors.
- Budget: Finasteride often wins on price when you’re on the NHS. Saw palmetto is the cheapest, but offers modest results.
- Prescription willingness: Minoxidil and saw palmetto are OTC; dutasteride and finasteride require a doctor’s script.
- Medical history: Men with liver impairment should avoid dutasteride, which is metabolised heavily by the liver.
Real‑world scenarios
Case 1 - 45‑year‑old man with mild BPH and early hair thinning: He started dutasteride 0.5mg daily. After six months, his urinary flow improved by 35% and his hair count rose 28%. He reported occasional decreased libido, which resolved after a two‑week holiday from the drug.
Case 2 - 30‑year‑old professional wary of hormonal changes: He chose 5% minoxidil foam twice daily and added saw palmetto supplements. After a year, his hair density increased by 12% with no sexual side effects. He continues to monitor scalp health with a dermatologist.
Case 3 - 60‑year‑old with severe BPH, no hair concerns: His urologist prescribed dutasteride 0.5mg. Within three months his prostate volume shrank by 15% and he no longer needed nightly bathroom trips. Because hair loss wasn’t an issue, no other medication was needed.
Tips for minimizing side effects
- Take the pill with food to reduce gastrointestinal upset.
- Schedule a follow‑up blood test at three months to check PSA and liver enzymes.
- If sexual dysfunction appears, discuss a temporary drug holiday with your doctor.
- Combine low‑dose minoxidil with an oral inhibitor for additive hair‑growth benefits, but check for scalp irritation.
Frequently Asked Questions
Is dutasteride approved for hair loss in the UK?
No. Dutasteride is licensed for BPH, but many specialists prescribe it off‑label for androgenetic alopecia based on its stronger DHT suppression.
How long does it take to see results with dutasteride?
Hair‑growth improvements typically appear after 4-6months of continuous use, with maximal benefit around 12months.
Can I use dutasteride and finasteride together?
Combining the two offers no added clinical benefit and raises the risk of side‑effects, so doctors generally advise against it.
Is saw palmetto a safe substitute for dutasteride?
Saw palmetto is much milder; it may help early‑stage hair loss but cannot replace dutasteride’s potency for BPH or severe alopecia.
What monitoring is required while on dutasteride?
Doctors usually order PSA, liver function tests, and lipid panels at baseline and then every 6‑12months.




Reading through the comparison makes me think about the broader philosophy of medical choices – balancing efficacy, cost, and personal values 😊. The dual inhibition of dutasteride indeed offers a broader reach, but the trade‑off is a higher side‑effect profile. For someone juggling both BPH and thinning hair, the convenience of a single pill can be a game‑changer. Yet, one must weigh the potential for sexual dysfunction against the benefits. In the end, it’s a personal calculus that each patient must perform.
Great rundown! It really helps to see the numbers side by side so you can make an informed decision.
When evaluating therapeutic options, one must consider not only efficacy, but also tolerability; indeed, the spectrum of adverse events varies considerably,; the pharmacokinetic profile of dutasteride, for example, suggests a prolonged half‑life, which may influence adherence; conversely, minoxidil requires twice‑daily application, a regimen that some patients might find burdensome.
Whoa, talk about a drug that’s a Swiss‑army knife! Dutasteride’s like that friend who shows up to every party-hair, prostate, you name it. But don’t forget the flip side: it can turn your love life into a sitcom episode. If you’re okay with a little drama, go for the powerhouse; otherwise, keep it simple and stick with the classics.
It is commendable how the table lays out the data, however there are a few minor errors that could be addrressed. For instance, the cost range for dutasteride appears a bit broad. Also, the mention of liver metabolism should be spelled as "metabolised" not "metabolized" if we keep it UK‑centric.
Dutasteride seems powerful but its drama is not for the faint‑hearted. Less punctuation here – just facts. It blocks both isoenzymes, so DHT drops sharply. Side effects can be a nightmare for some; yet many tolerate it well. The cost is steep though, especially off‑label. Choose wisely.
Let us begin by acknowledging the comprehensive nature of the comparison presented; it offers a solid foundation for clinical decision‑making. The data summarise that dutasteride exerts a broader inhibition of 5‑alpha‑reductase, encompassing both type I and type II isoenzymes, which translates into a greater reduction in systemic DHT levels. This pharmacodynamic profile accounts for the observed superiority in both hair‑regrowth metrics-approximately a 30‑45% increase in hair count-and prostate volume reduction, as evidenced by multiple randomized controlled trials. In contrast, finasteride, while effective, targets only type II, yielding a comparatively modest DHT suppression of roughly 70%, and correspondingly lower efficacy in the two therapeutic domains.
From an adverse‑event perspective, the broader enzymatic blockade of dutasteride introduces a marginally higher incidence of sexual dysfunction, including decreased libido, erectile dysfunction, and ejaculatory disorders. These effects, though clinically significant, are often reversible upon discontinuation or dose reduction. Finasteride shares a similar side‑effect spectrum but at a slightly reduced frequency, which may be a deciding factor for patients particularly concerned about sexual health. Minoxidil, as a topical agent, bypasses systemic hormonal pathways, thereby eliminating sexual side effects; however, it is limited by its modest efficacy (10‑25% hair‑count increase) and potential for local irritation or unwanted facial hair growth.
Economic considerations cannot be ignored. The presented cost analysis illustrates that dutasteride, when prescribed off‑label for alopecia, incurs a higher out‑of‑pocket expense (up to £90 per month) compared with finasteride (£15‑£25 on the NHS). Minoxidil and saw palmetto remain the most affordable options, though their clinical potency is inferior. Patients with constrained budgets may therefore prioritize finasteride for combined BPH and hair‑loss management, reserving dutasteride for cases where maximal efficacy outweighs financial and side‑effect concerns.
In practical terms, the decision algorithm should weigh three primary axes: therapeutic goal (BPH, hair loss, or both), tolerability profile, and budgetary constraints. For a patient seeking concurrent management of moderate BPH and early‑stage androgenetic alopecia, dutasteride offers the most comprehensive solution, provided they are counseled on potential sexual side effects and monitored with periodic PSA and hepatic panels. Those with isolated hair‑loss concerns and a low tolerance for hormonal modulation may opt for minoxidil, possibly supplemented with saw palmetto, while retaining finasteride as a cost‑effective alternative when the budget permits. Ultimately, shared decision‑making, informed by the robust data presented, remains the cornerstone of optimal patient care.
Wow, that was a wall of text – impressive, but also a bit overwhelming :). I get that dutasteride is powerful, yet the side‑effects can be a real buzzkill. If you’re not into the drama, stick with minoxidil or a low‑dose finasteride. Just remember, no magic pill, you still need patience.
It’s good to have options, but the real world experience often diverges from trial data. I’ve seen patients who can’t tolerate dutasteride’s side effects, even at low doses, while others do just fine. The key is a personalized approach and proper monitoring.
The article leans heavily on dutasteride’s superiority without adequately addressing the long‑term safety concerns. One could argue that the enthusiasm is overblown and that more conservative options deserve equal scrutiny.
Sure, dutasteride looks shiny, but remember the side‑effects can be a nightmare.
Thanks for the clear breakdown! It’s helpful to see the pros and cons laid out side by side. I’ll discuss these options with my doctor at the next visit.
Drama alert! Dutasteride is like the superhero of hair loss meds – flying in to save the day, but sometimes it forgets to bring the cape of side‑effect safety.
This comparison is overly optimistic about dutasteride. In practice the patient adherence drops due to the unpleasant side effects, making it less effective than the charts suggest.
I love how the article gives a full picture – it’s not just about the wins, but also the “uh‑oh” moments. It’s refreshing to see a balanced view that respects both the science and the patient’s lived experience. Keep the thorough analysis coming! It helps everyone make smarter choices.
From a national perspective, we must prioritize cost‑effective treatments that benefit the broader population. Dutasteride’s high price limits accessibility, and we should focus on proven, affordable alternatives.
👍
The data are presented with excellent clarity; it’s a solid reference for both clinicians and patients. I appreciate the precise language and comprehensive coverage. Well done on a thorough piece.
Loved the comparative tables 😍 – they made the differences pop right off the screen! The emojis sprinkled throughout kept it lively and easy to digest.
The overview is useful, though I’d like to see more on patient adherence rates. Also, a note on hepatic monitoring would be valuable for clinicians.